| E-Briefings – Volume 22, No. 4, July 2025 |
|
Download the full PDF →
An Interview with Dr. G: Combating the Digital Spread of Misinformation →Geeta Nayyar, M.D., M.B.A., Chief Medical Officer, Technologist, and Best-Selling Author TGI: Let’s start by discussing the misinformation problem that we are having in healthcare. What is amplifying this and how can it harm patients, families, and communities? Dr. G: First, it’s important to recognize that misinformation and disinformation are not new problems in healthcare, but they are getting worse because of the era of technology we are living in with social media and AI, as well as a post-pandemic consumer who is hungry for healthcare information. One in four Americans go on social media at least weekly to look up information about their health, and misinformation is traveling six times faster than the facts. This is no longer something healthcare boards and senior leadership can ignore. In this tech-forward society, it is easier to engage and inspire the average consumer in a way that healthcare doesn’t. When we look at how payers and hospitals typically engage their patients, it’s often generic and tied to a milestone, such as a birthday postcard or a congratulatory note after the birth of a baby. This is very different than what we experience on TikTok or Instagram where algorithms provide a customized experience to each consumer. These platforms know exactly who you are, what you like, and the types of people that you follow. The most important thing to recognize is that healthcare now faces real competition on social media. Hospitals are no longer competing with just the hospital or clinic down the street—they are competing with influencers, too. These influencers know the healthcare system and process itself is cumbersome and promote easier, cheaper solutions, such as a home genetic kit for $99 that detects if you will get breast cancer, in place of a mammogram where you would have to make an appointment and pay a co-pay. The challenge with healthcare on social media is that it’s often driven by entertainment rather than expertise, which means the information shared isn’t always accurate. But that is where consumers are turning for information, and if hospitals remain silent or limit their outreach to a postcard, they won’t be able to compete. Patient acquisition, retention, and brand loyalty requires an omni-channel approach—combining social media, billboards, direct mail, personal outreach, phone calls, and text messaging to meet people where they are. Limiting the spread of misinformation and disinformation is no longer just a moral imperative; it is a business problem. Consumers are delaying hospital visits, skipping tests and screenings, and avoiding preventative care, and that is jeopardizing patient outcomes and resulting in lost revenue for hospitals.
TGI: As healthcare organizations, how can we better capture people’s attention on social media? What lessons can we take from influencers to leverage algorithms effectively and make science-based health information more accessible and engaging for everyday Americans? Dr. G: The first step is ensuring the Chief Marketing Officer and Chief Medical Officer are closely aligned and collaborating on this effort. Too often, these roles operate in silos and are not working together to drive strategy or input. The Mayo Clinic and Cleveland Clinic are two use cases demonstrating the power of this partnership. Their trusted brands, extensive content libraries, and sophisticated digital strategies have allowed them to consistently outperform algorithms and effectively engage audiences across platforms. Next, make sure your Chief Marketing Officer and Chief Medical Officer are regularly meeting to discuss clinical challenges and explore how marketing strategies can help address them. A current example is tackling misinformation around measles if there is an outbreak in your area. Start by auditing where misinformation and disinformation are circulating and assess your brand’s reputation in the community. Survey patients to learn where they seek out and engage with healthcare information. Then use these insights to develop a targeted outreach strategy. Part of the strategy execution will be engaging your doctors, nurses, and workforce. There are naturally amazing influencers and communicators on hospital staffs. In fact, some of your doctors and nurses may already be doing this on their own because it’s driving business to their clinic or strengthening their own brand. Hospitals can collaborate with these clinicians to create content and amplify their influence on social media. Then, after you execute that strategy, review the metrics: does it boost trust? Is it increasing the number of patient visits? There is a business case behind getting this strategy right. When it is executed with the C-suite—the Chief Medical Officer, Chief Marketing Officer, Chief Financial Officer, Chief Information Officer, and Chief Technology Officer—the content strategy can drive patient visits, both brick-and-mortar and virtually, and boost revenue. TGI: Some boards may feel like this is too far out of the not-for-profit hospital or health system’s scope. Why should boards pay attention to this and ensure that their organizations are educating the public and combating misinformation and disinformation? Dr. G: Boards have a fiduciary responsibility to their hospitals and this affects their business. This is about staying viable in today’s healthcare environment. We all saw what misinformation and disinformation did to hospitals through the pandemic, both from a staff morale and patient volume standpoint. People put off going to the hospital, not just because of capacity issues but because they were not convinced the science could be trusted. Then when life-saving measures became available, we couldn’t get anyone to take them. There is a business case here and misinformation and disinformation are likely affecting the bottom line, but it has not necessarily been measured. With the path we are on now, with even public health leadership spreading information that is not sound science, the onus is going to fall on hospitals to really justify why people need to go to the hospital in the first place. The wellness movement is taking over and becoming a lot more mainstream than actually dealing with chronic disease management and illness. Because of this shift, we are going to be seeing sicker patients—those patients that avoid care or get care too late when the supplements don't work and the home genetic kits fail. If you are providing value-based care, patient engagement and education is key, including working with marketing on the social media piece. Patients won’t come in for preventative treatments and screenings if they don’t understand and believe in the necessity.
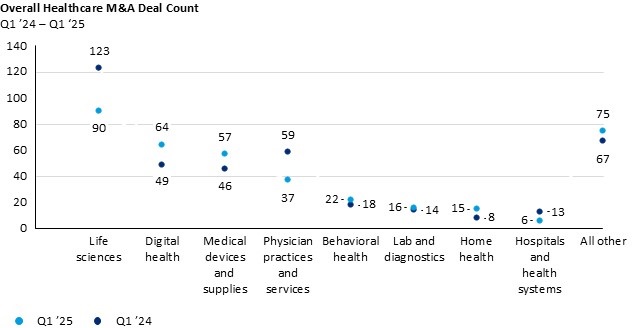
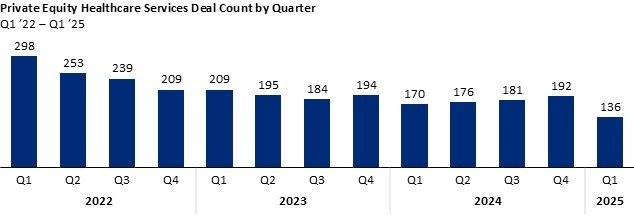
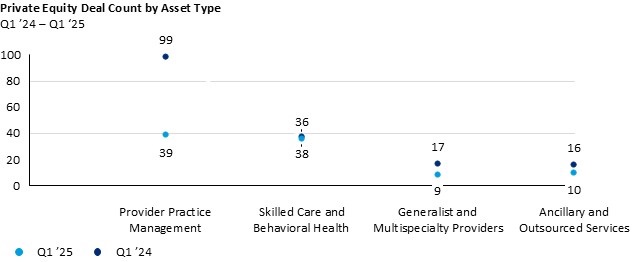
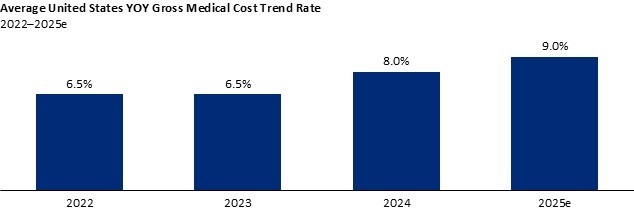
TGI: What are some strategic conversations boards can be having about this with senior leadership and physician leaders? Dr. G: First is asking the questions. Have we studied the effects of misinformation and disinformation in our community? Is it affecting our bottom line? Do consumers and staff trust our hospital’s brand? If revenues are going down, whether it is preventative screenings or visits to the ambulatory clinic, this could be one of the data points you are not looking at. Separate but parallel is the workforce issue and how this misinformation can contribute to physician burnout. For example, if you ask pediatricians what the hospital can do to help with the back-to-school season, many will say they need assistance combatting the disinformation around vaccines. Doctors do not want to spend eight minutes of the visit convincing families and patients about the effectiveness of vaccines. Staff will appreciate the hospital leadership recognizing the environment and how demoralizing it can be and stepping up to provide digital tools (such as a YouTube channel) to help scale these conversations with patients. Lastly, building strong community relationships should also go hand in hand with the digital solutions to combating misinformation. Places like churches, temples, barber shops, and other local gathering spaces play a critical role in fostering trust, particularly in communities where skepticism about the healthcare system persists. As hospitals build their outreach strategies, they should prioritize keeping these relationships strong. It’s also essential to understand what is truly happening in these communities—whether people are coming to the hospital, why they might be avoiding it, and what concerns or barriers exist. Bringing these conversations into the boardroom will position boards to better support and champion strategies designed to combat misinformation, strengthen public confidence, and protect the organization’s reputation. Private-Equity Healthcare M&A: Ongoing Volatility Pushes Investors to Concentrate in Key Sectors →By Kevin Wistehuff, Principal; Luke Marazzo, Engagement Manager; Noah Piwonka, Associate; Michael Chen, Associate; Deepika Bangia, Senior Research Analyst; and Emily Lin, Research Intern; Oliver Wyman As the U.S. healthcare sector continues its post-pandemic realignment, hospital and health system leaders are navigating increasingly segmented M&A dynamics. Q1 2025 data shows that deal activity varies significantly by sector, with hospital transactions reaching historic lows while digital health and home-based care continue to attract private capital. This article provides a fact-based synthesis of current trends with implications for governance, strategic planning, and operational resilience. Industry-Wide TrendsModest Decline in Healthcare M&A through Q1 While transactions in home care, digital health, and staffing experienced growth in Q1 2025, the segment overall posted a 3.8 percent decline compared to the same quarter in 2024. Sectors such as pharmaceuticals, physician practices, and hospitals contributed to this drop, with 27 percent, 38 percent, and 54 percent declines respectively in total deal activity. Source: Modern Healthcare, Oliver Wyman analysis. Private Capital Activity Slows Dramatically, with Heavy Concentration in Key Sectors Private-equity-backed deal count declined a significant 23 percent in Q1 2025 from Q1 2024. While declines were felt across all asset types, the biggest contributor to slowdowns was the physician practice management sector, which experienced a 61 percent decrease in total deals. Source: PitchBook, Oliver Wyman analysis. Source: PitchBook, Oliver Wyman analysis. Macroeconomic Trends The U.S. Federal Reserve’s late 2024 rate cuts have stabilized financing conditions, with light expectations of further cuts by Q4 2025, creating a potential for accelerated deal activity. However, ongoing policy and market volatility have caused some hesitancy to move ahead with major investments or acquisitions. Finally, continued and accelerating medical inflation is pressuring plans, providers, and employers, creating opportunities to deliver value through more effective cost control. Source: Aon Global Medical Trends Rate Report, Oliver Wyman analysis.
Key Board Takeaways
Sector-Specific Points of InterestDigital Health Remains a Key Investment Priority Multiple high-profile digital health fundraises were reported in Q1, including:
Firms with successful fundraises in the recent quarter tended to report partnerships with health systems or payers, demonstrating a trend toward integrated digital-care infrastructure. Significant Consolidation in Staffing Services Increased consolidation is underway in the healthcare staffing sector. There have been multiple transactions, including Aya Healthcare’s $615 million acquisition of Cross Country Healthcare and All Star Healthcare Solutions’ acquisition of Integrity Locums. Executives attribute the trend to reduced post-pandemic demand and declining bill rates. April Hansen, CEO of Barton Associates, commented on this saying, “We’re seeing consolidation as a necessary path forward to remain competitive.” Hospital M&A Slows Dramatically, with Emphasis on Financial Distress Kaufman Hall reported only five announced hospital transactions in Q1 2025, compared to 20 in Q1 2024. Four of the five transactions involved distressed assets, with no mega-mergers observed. The average annual revenue of acquired hospitals dropped to $279 million—half of 2024’s average. However, Ascension Health was one exception; the system transitioned from divestitures to strategic acquisitions, including a $460 million deal for Cedar Park Regional Medical Center in Texas. Ascension also expanded its outpatient portfolio via joint ventures. Key Industry News and TrendsIncreased Regulatory Scrutiny Regulatory oversight intensified, as Oregon legislators passed a bill to restrict private-equity ownership in medical practices, particularly via management services organizations (MSOs). Oregon Public Broadcasting (OPB) reports that the bill—awaiting the governor’s signature—could set a precedent for broader state-level regulation. In addition, at least nine states have introduced proposals to strengthen transaction review and approval regimes, creating heightened requirements for private-equity investors or private-equity-backed providers. Healthcare leaders should monitor similar legislative trends in California, New York, and Massachusetts, where comparable bills are in preliminary stages. Growing Cross-Border Innovation, Despite Political Environment The Wall Street Journal documented a growing trend: U.S. pharmaceutical companies increasingly license late-stage compounds from Chinese biotech firms. In 2023–2024, 30 percent of Big Pharma licensing activity involved China-developed drugs—up from 12 percent in 2021–2022. Pfizer’s $6 billion licensing agreement with Chinese biotech firm, 3Sbio, and Avenzo’s oncology deal with Duality Biotherapeutics highlight a move to diversify research and development pipelines. Key Deals Highlight Investor Focus on Specialized Populations and Tech Integration Two key transactions in Q1 2025 illustrate prevailing themes:
Both deals reflect strategic interest in value-based care, tech integration, and high-need populations. Final Thoughts: M&A Is Not Uniform, But Strategy Must BeIn 2025, healthcare M&A and private capital activity reflect divergence rather than decline. Hospital boards and executives must adopt sector-aware, data-driven strategies—recognizing where capital is flowing and why. By remaining agile and informed, governance teams can pursue mission-aligned growth without assuming undue risk. 2025 will not reprise the frothy days of 2021, but it will be a year in which disciplined capital meets a healthcare system ripe for transformation. In this new era, the winners will be those who embrace innovation, forge strategic partnerships, and maintain a relentless focus on operational excellence. TGI thanks Kevin Wistehuff, Principal, Luke Marazzo, Engagement Manager, Noah Piwonka, Associate, Michael Chen, Associate, Deepika Bangia, Senior Research Analyst, and Emily Lin, Research Intern, at Oliver Wyman, for contributing this article. They can be reached at kevin.wistehuff@oliverwyman.com. Learning Health Networks: A Hidden Asset for Boards →By Daniel Hyman, M.D., M.M.M., Founder and Principal, Frontline Quality Solutions, and Peter Margolis, M.D., Ph.D., Co-Director Emeritus, James M. Anderson Center for Health Systems Excellence at Cincinnati Children's Hospital Medical Center
Key Questions for Board Members to Ask About Learning Health Networks
Directors of hospital boards have an opportunity to help the healthcare organizations they serve make meaningful progress on some of healthcare’s most persistent challenges: dramatically reducing preventable harm, improving survival in rare conditions, and enabling more patients to live well with chronic illness. Across the country, a growing number of hospitals are realizing these breakthroughs through an emerging way of accelerating large-scale improvement known as the Learning Health Network (LHN), a highly impactful approach to improvement that remains underutilized in our healthcare system. What Is a Learning Health Network?LHNs are working communities of patients and families, clinicians, and researchers collaborating at scale toward the shared goal of better health. In an LHN, all participants—patients, families, clinicians, and researchers—work together to identify and solve problems. LHNs empower small teams of clinicians and others to collaborate across organizational boundaries to rapidly improve care. They enable patients, families, and clinicians to work together to reveal insights and create innovative solutions to problems that are not being solved through traditional care models or other standard improvement efforts. They help large hospitals caring for hundreds of thousands of patients discover what works for which patients, enabling personalized care. Transparent, shared data on outcomes and care are used to guide clinical decisions, catalyze care improvements, and accelerate clinical research. Each encounter within an LHN is an opportunity to generate evidence and collaborate for evidence-based, personalized decisions. LHNs are not a new technology, but a way of building action-oriented communities that work together to solve complex challenges. Most importantly, LHNs have proven effective at improving health outcomes for patients. A children’s hospital safety network with 145 participating organizations has reduced serious safety events by more than 30 percent, spared more than 30,000 children from hospital-acquired harm, and saved almost $700 million (as of February 2025). A network focused on rare single-ventricle congenital heart disease reduced patient mortality by 40 percent. Hospitals participating in a network focused on improving care for Crohn’s Disease and ulcerative colitis increased the percentage of patients in remission from 60 to 83 percent. The American Board of Pediatrics spawned the model of the LHN. These three networks are among more than a dozen comparable examples that demonstrate the benefit and the potential of LHNs across healthcare organizations, and for that matter, across other sectors, including education and public health.
The Case for LHNs in Healthcare TodayDespite extraordinary advances in medicine, technology, and science, the U.S. healthcare system continues to deliver uneven results—marked by inefficiencies, uneven access, and frustratingly slow adoption of proven innovations. As Dr. Paul Batalden observed, “Every system is perfectly designed to achieve exactly the results it gets.” To achieve different results, we must organize care differently. Healthcare is growing more complex every day. Patients face increasingly fragmented care. Clinicians lack the time, tools, and timely data to make the best, evidence-based decisions for each individual. Payers, providers, and purchasers often pursue goals in isolation, and promising research discoveries may take years to influence practice—if they do at all. Meanwhile, new treatments and technologies, including artificial intelligence, are emerging at an unprecedented pace. But without better mechanisms to align goals, harness distributed expertise, and translate knowledge into action, these advances won’t reliably reach the patients who need them. This is precisely where LHNs come in. LHNs create data-driven, outcome-focused collaboration across healthcare organizations—linking patients, clinicians, researchers, and institutions as communities that learn and improve together. Some directors may have heard the term and/or support organizations that consider themselves to be a “Learning Health System.” For almost 20 years, the National Academy of Medicine has promoted the vision of a Learning Health System “in which science, informatics, incentives, and culture are aligned for continuous improvement, innovation, and equity—with best practices and discovery seamlessly embedded in the delivery process, individuals as active participants in all elements, and new knowledge generated as an integral by-product of the delivery experience.” LHNs have brought the vision to life at scale through shared data, shared learning, and shared accountability for results. Strategic collaboration is not unique to healthcare. Across industries, organizations are responding to complexity and rapid change by forming collaborative networks. For example, in commercial aviation, competitors like Delta, United, and American collaborate to share data, align standards, and continuously improve safety and efficiency. They compete in the marketplace, but cooperate on systems where shared success matters. Healthcare, facing a similarly high-stakes and fast-evolving landscape, must adopt the same mindset—working together where it improves outcomes, builds trust, and reduces waste. Importantly, LHNs also position organizations for success in the evolving payment environment. As reimbursement increasingly shifts toward value and outcomes, rather than volume, health systems will need better ways to demonstrate quality, reduce harm, and manage chronic conditions across populations. LHNs provide the infrastructure and peer collaboration to meet these goals with rigor and transparency. While pioneered in pediatrics, LHNs are increasingly being developed for adult chronic and complex conditions. They support transparency, reduce duplication of effort, and help systems learn faster than any could alone. For hospital boards, LHNs represent a timely and strategic way to fulfill core responsibilities—quality, stewardship, and innovation. TGI thanks Daniel Hyman, M.D., M.M.M., Founder and Principal, Frontline Quality Solutions, and Peter Margolis, M.D., Ph.D., Co-Director Emeritus, James M. Anderson Center for Health Systems Excellence at Cincinnati Children's Hospital Medical Center, for contributing this article. They can be reached at danhyman2@gmail.com and peter.margolis@cchmc.org. For a deeper dive on this topic, check out IHI’s Turn on the Lights podcast, where they explore LHNs as a powerful, cost-effective strategy for improving healthcare outcomes through collaboration. |
The Governance Institute
1245 Q Street
Lincoln, NE 68508
1.877.712.8778